2.3.2.1 Introduction
1.Etiology and pathogenesis
(1)Risk factors:Ultraviolet(UV)radiation is the main environmental risk factor.Host risk factors for melanoma include the presence of melanocytic or dysplastic naevi,a personal history of melanoma,a family history of melanoma,and phenotypic characteristics including fair hair,eye and skin colors,and the tendency to freckle.Gene mutations account for only a small proportion of melanoma cases.
(2)The genesis of melanoma:UVA radiation induces melanocytes malignant transformation through two different mechanisms.The direct transformation of normal melanocytes in neoplastic cells through the occurrence of several mutations affecting both proto-oncogene and tumor suppressor genes(TP53,NF1,PTEN,etc.).The activating BRAF mutation is a typical feature of benign nevi formation and BRAF is mutated in up to 80%of benign nevi.These nevi remain indolent for decades due to immune surveillance.Further progression into intermediate lesions,melanomas in situ,invasive potential and metastasis requires additional mutations.The most frequent somatic mutations affect genes that control central cellular process,such as proliferation(BRAF,NRAS and NF1),growth and metabolism(PTEN and KIT),resistance to apoptosis(TP53),cell cycle control(CDKN2A)and replicative lifespan(TERT).These genetic alterations yield a reciprocal overstimulation of the affected cellular pathways in melanoma,mainly the MAPK pathway and the PI3K/AKT pathway.
(3)Tumor microenvironmental alterations:Melanoma spreading is the result of genetic mutations and tumor microenvironmental alterations.A key role is played by the overexpression of matrix metalloproteinases(MMPs)that induces the degradation of the components of the extracellular matrix to favor tumor cell infiltration and spreading through the bloodstream.
(4)Immune escape of melanoma cells:Melanoma cells also evade the immune system.Upon tumor antigen recognition by T cells,released interferons trigger JAK-STAT-mediated expression of PD-1 ligands PD-L1 and PD-L2 on the surface of melanoma cells.Binding of PD-L1 and PD-L2 to PD-1 leads to the suppression of T cell activity and inhibits the antitumor immune response.Further immunosuppressive mechanisms include the down regulation of tumor-associated antigens and class Ⅰ major histocompatibility complex,and the secretion of inhibitory factors like tumor growth factor-β.
2.Clinical presentations,subtypes and staging
(1)Clinical presentations and subtypes:Typical features are asymmetry of the lesion,irregular borders,inhomogeneous color,diameter of 5 mm and more.
①Superficial spreading melanoma(57.4%):Common in trunk in men and lower legs in women.It begins as macule with slow radial growth phase limited to epidermis or focally in papillary dermis and then develops into papule or nodule with a rapid vertical growth phase.On dermoscopy,it exhibits broad network of multiple brown dots,color variation and possible depigmentation.Histologically,the feature is pagetoid spread of malignant melanocytes throughout the epidermis(Figure 2-10).
②Nodular melanoma(21.4%):Typically arises on trunk,head and neck in men more than women.It begins as a blue black,or pink nodule which may ulcerate or bleed with an aggressive vertical phase and a short or absent horizontal growth phase.On dermoscopy,it exhibits individual globules with color variation,white streaks and irregular vessels.Microscopically,there are irregular nests of melanocytes.
③Lentigo maligna melanoma(8.8%):Common in nose,cheek,or any sun-damaged skin.It begins as a brownish black macule with variegated color and irregular indented border.On dermoscopy,it exhibits hyperpigmented follicular openings slowly overgrown by irregular pigmented dots.It is characterized histologically by a lentiginous proliferation of atypical melanocytes at the dermal-epidermal junction and histological features of solar elastosis.
④Acral lentiginous melanoma(4%):Commonly arises on soles and palms.In its initial intraepidermal phase,there is irregular and poorly circumscribed macule;therewith a nodular region reflects the invasive growth pattern.On dermoscopy,it exhibits irregular,gray-brown polygons and multiple hypopigmented areas.When involving the nail bed,it can present with longitudinal melanonychia extending onto the hyponychium or beyond the lateral or proximal nail fold,the latter referred to as Hutchinson's sign.Histologically,there are proliferating and atypical melanocytes within basal layer of hyperplastic dermis either arranged solitary or in irregular nests.
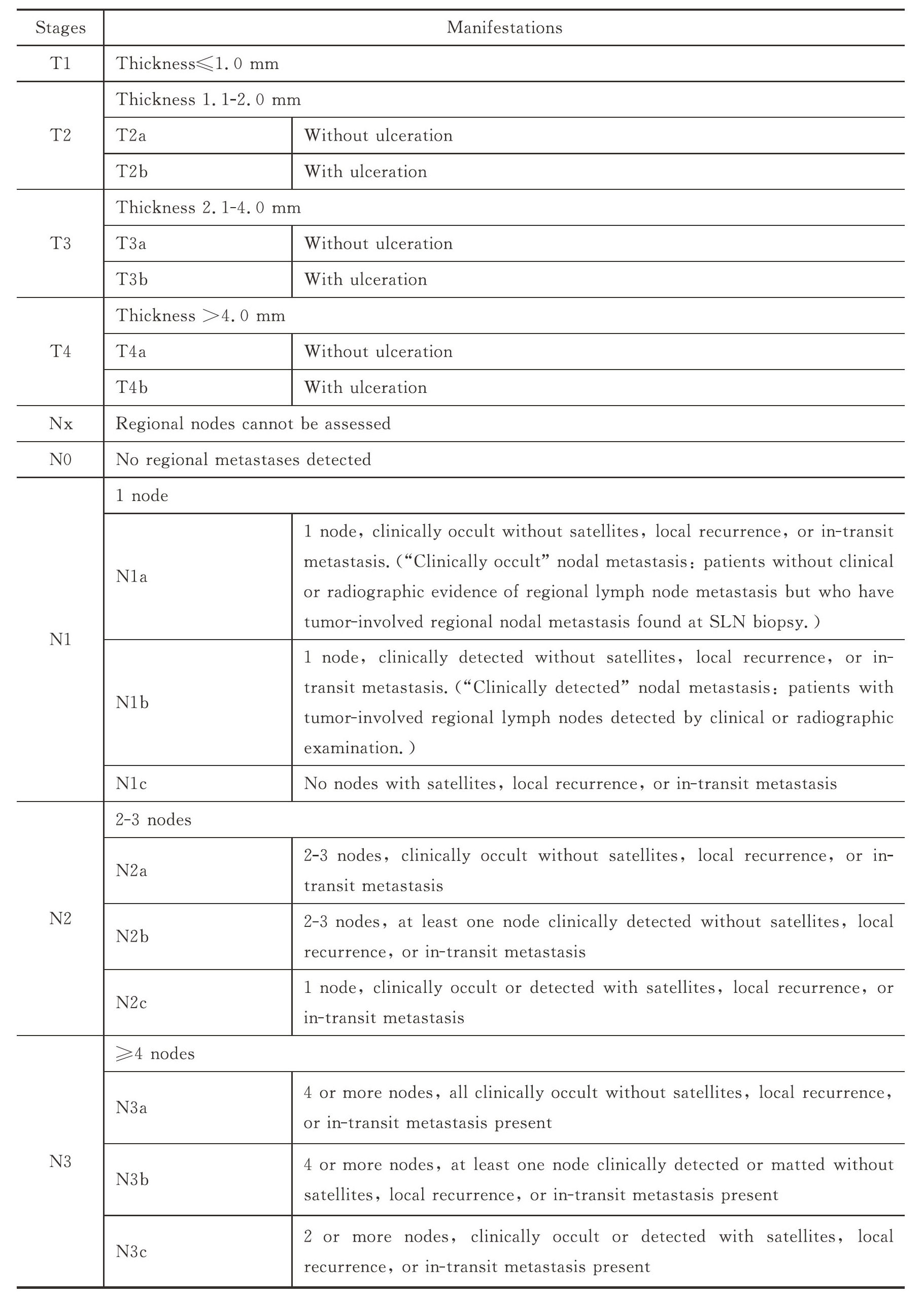
(2)TNM classification:AJCC 8th edition TNM staging categories for melanoma,see Table 2-1.
Table 2-1 TNM staging for melanoma

Continued
Continued

(3)Clinical staging and pathologic staging of melanoma see Table 2-2.
Table 2-2 Clinical staging and pathologic staging of melanoma

Continued

3.Diagnosis and differential diagnosis
(1)Clinical and dermoscopic diagnosis:Most melanomas are readily detected and diagnosed by visual inspection by an experienced physician because of their prominent pigmentation and morphological pattern.People at an increased risk for melanoma should be screened at regular intervals.High-risk characteristics that prompt screening or surveillance include melanocytic naevi,dysplastic naevi,and personal and family histories of melanoma.Screening for melanoma includes a total body skin examination supported by dermoscopy or other imaging techniques.
Examination with the naked eye assesses the so-called A(asymmetry),B(irregular borders),C(inhomogeneous color)and D(diameter ≥5 mm)criteria,which point to suspicious melanocytic lesions(ABCD rule).
Dermoscopy is an essential tool for the examination of pigmented and non-pigmented skin tumors to detect melanoma.Melanoma-specific criteria includes atypical pigment network,irregular dots/globules,irregular streaks,blue-whitish veil,regression structures,irregular vascular structures,blotches,shiny white streaks and rosettes.
The differential diagnosis of melanoma involves other melanocytic pigmented lesions(congenital,atypical,common melanocytic naevi and actinic lentigo),non-melanocytic pigmented lesions(seborrheic keratosis,hemangioma,dermatofibroma,and pigmented basal cell carcinoma),and other non-pigmented tumors(hemangioma,basal cell carcinoma,squamous cell carcinoma).
(2)Histopathologic diagnosis:Histological examination can provide information about clinic-pathologic type,tumor thickness,presence or absence of ulceration,mitotic activity,microsatellites,lateral and deep excision margins,vascular or perineural involvement.
(3)Immunohistochemical stains:Characteristic markers commonly used for melanocytes include S100,SOX10,MART1/Melan-A,HMB45,tyrosinase,MITF and Ki67.A mixture of two or more markers can be used in immunohistochemistry to increase the sensitivity for the detection of melanocytes.The markers of melanocytic differentiation include S100,MART1/Melan-A,HMB45,tyrosinase,MITF and SOX10.The sensitivity of S100 in melanomas is very high,which makes it a screening index,but the specificity of S100 is not high.MART1/Melan-A,HMB45 and tyrosinase have high specificity.MITF and SOX10 are useful markers for the distinction of pigmented actinic keratosis from melanoma in situ.Prognostic markers of melanoma include Ki67 and phosphohistone H3(PHH3).In melanomas,the Ki67 proliferation index ranges from 5%-50%,with mitotic figures distributed throughout the lesion.
(4)Molecular diagnosis:The main molecular diagnosis test performed involves the BRAF V600 mutational status,to identify patients eligible for treatment with BRAF inhibitors and MEK inhibitors.NRAS mutations,NF1 mutations and CKIT mutations have also been identified in a proportion of cases.Cellular and molecular methods that have been applied to the diagnosis of melanoma include comparative genomic hybridization(CGH),fluorescence in situ hybridization(FISH),imaging mass spectrometry(IMS),quantitative real-time polymerase chain reaction(qRT-PCR),multiplex ligation-dependent probe amplification(MLPA).
(5)Imaging diagnosis:Ultrasonography of the regional lymph-node and radiographic imaging using CT or MRI should be done to exclude metastatic spread.
(6)Other imaging techniques:Other imaging techniques are available to assist the physicians in the differentiation of melanoma and its precursors from benign lesions,which include in vivo reflectance confocal microscopy,computer-aided multispectral digital analysis,electrical impedance spectroscopy(EIS),photoacoustic imaging(PAI),and optical coherence tomography.